
Pain
Definition
Pain is an unpleasant feeling that is conveyed to the brain by sensory neurons. The discomfort signals actual or potential injury to the body. However, pain is more than a sensation, or the physical awareness of pain; it also includes perception, the subjective interpretation of the discomfort. Perception gives information on the pain’s location, intensity, and something about its nature. The various conscious and unconscious responses to both sensation and perception, including the emotional response, add further definition to the overall concept of pain.
Description
Pain arises from any number of situations. Injury is a major cause, but pain may also arise from an illness. It may accompany a psychological condition, such as depression, or may even occur in the absence of a recognizable trigger.
Acute pain
Acute pain often results from tissue damage, such as a skin burn or broken bone. Acute pain can also be associated with headaches or muscle cramps. This type of pain usually goes away as the injury heals or the cause of the pain (stimulus) is removed.
To understand acute pain, it is necessary to understand the nerves that support it. Nerve cells, or neurons, perform many functions in the body. Although their general purpose, providing an interface between the brain and the body, remains constant, their capabilities vary widely. Certain types of neurons are capable of transmitting a pain signal to the brain.
As a group, these pain-sensing neurons are called nociceptors, and virtually every surface and organ of the body is wired with them. The central part of these cells is located in the spine, and they send threadlike projections to every part of the body. Nociceptors are classified according to the stimulus that prompts them to transmit a pain signal. Thermoreceptive nociceptors are stimulated by temperatures that are potentially tissue damaging. Mechanoreceptive nociceptors respond to a pressure stimulus that may cause injury. Polymodal nociceptors are the most sensitive and can respond to temperature and pressure. Polymodal nociceptors also respond to chemicals released by the cells in the area from which the pain originates.
Nerve cell endings, or receptors, are at the front end of pain sensation. A stimulus at this part of the nociceptor unleashes a cascade of neurotransmitters (chemicals that transmit information within the nervous system) in the spine. Each neurotransmitter has a purpose. For example, substance P relays the pain message to nerves leading to the spinal cord and brain. These neurotransmitters may also stimulate nerves leading back to the site of the injury. This response prompts cells in the injured area to release chemicals that not only trigger an immune response, but also influence the intensity and duration of the pain.
Chronic and abnormal pain
Chronic pain refers to pain that persists after an injury heals, cancer pain, pain related to a persistent or degenerative disease, and long-term pain from an unidentifiable cause. It is estimated that one in three people in the United States will experience chronic pain at some point in their lives. Of these people, approximately 50 million are either partially or completely disabled.
Chronic pain may be caused by the body’s response to acute pain. In the presence of continued stimulation of nociceptors, changes occur within the nervous system. Changes at the molecular level are dramatic and may include alterations in genetic transcription of neurotransmitters and receptors. These changes may also occur in the absence of an identifiable cause; one of the frustrating aspects of chronic pain is that the stimulus may be unknown. For example, the stimulus cannot be identified in as many as 85% of individuals suffering lower back pain.
Scientists have long recognized a relationship between depression and chronic pain. In 2004, a survey of California adults diagnosed with major depressive disorder revealed that more than one-half of them also suffered from chronic pain.
Other types of abnormal pain include allodynia, hyperalgesia, and phantom limb pain. These types of pain often arise from some damage to the nervous system (neuropathic). Allodynia refers to a feeling of pain in response to a normally harmless stimulus. For example, some individuals who have suffered nerve damage as a result of viral infection experience unbearable pain from just the light weight of their clothing. Hyperalgesia is somewhat related to allodynia in that the response to a painful stimulus is extreme. In this case, a mild pain stimulus, such as a pin prick, causes a maximum pain response. Phantom limb pain occurs after a limb is amputated; although an individual may be missing the limb, the nervous system continues to perceive pain originating from the area.
Causes and symptoms
Pain is the most common symptom of injury and disease, and descriptions can range in intensity from a mere ache to unbearable agony. Nociceptors have the ability to convey information to the brain that indicates the location, nature, and intensity of the pain. For example, stepping on a nail sends an information-packed message to the brain: the foot has experienced a puncture wound that hurts a lot.
Pain perception also varies depending on the location of the pain. The kinds of stimuli that cause a pain response on the skin include pricking, cutting, crushing, burning, and freezing. These same stimuli would not generate much of a response in the intestine. Intestinal pain arises from stimuli such as swelling, inflammation, and distension.
Diagnosis
Pain is considered in view of other symptoms and individual experiences. An observable injury, such as a broken bone, may be a clear indicator of the type of pain a person is suffering. Determining the specific cause of internal pain is more difficult. Other symptoms, such as fever or nausea, help narrow down the possibilities. In some cases, such as lower back pain, a specific cause may not be identifiable. Diagnosis of the disease causing a specific pain is further complicated by the fact that pain can be referred to (felt at) a skin site that does not seem to be connected to the site of the pain’s origin. For example, pain arising from fluid accumulating at the base of the lung may be referred to the shoulder.
Since pain is a subjective experience, it may be very difficult to communicate its exact quality and intensity to other people. There are no diagnostic tests that can determine the quality or intensity of an individual’s pain. Therefore, a medical examination will include a lot of questions about where the pain is located, its intensity, and its nature. Questions are also directed at what kinds of things increase or relieve the pain, how long it has lasted, and whether there are any variations in it. An individual may be asked to use a pain scale to describe the pain. One such scale assigns a number to the pain intensity; for example, 0 may indicate no pain, and 10 may indicate the worst pain the person has ever experienced. Scales are modified for infants and children to accommodate their level of comprehension.
Treatment
There are many drugs aimed at preventing or treating pain. Nonopioid analgesics, narcotic analgesics, anticonvulsant drugs, and tricyclic antidepressants work by blocking the production, release, or uptake of neurotransmitters. Drugs from different classes may be combined to handle certain types of pain.
Nonopioid analgesics include common over-the-counter medications such as aspirin, acetaminophen (Tylenol), and ibuprofen (Advil). These are most often used for minor pain, but there are some prescription-strength medications in this class.
Narcotic analgesics are only available with a doctor’s prescription and are used for more severe pain, such as cancer pain. These drugs include codeine, morphine, and methadone. Addiction to these painkillers is not as common as once thought. Many people who genuinely need these drugs for pain control typically do not become addicted. However, narcotic use should be limited to patients thought to have a short life span (such as people with terminal cancer) or patients whose pain is only expected to last for a short time (such as people recovering from surgery). In August 2004, the Drug Enforcement Administration (DEA) issued new guidelines to help physicians prescribe narcotics appropriately without fear of being arrested for prescribing the drugs beyond the scope of their medical practice. DEA is trying to work with physicians to ensure that those who need to drugs receive them but to ensure opioids are not abused.
Anticonvulsants, as well as antidepressant drugs, were initially developed to treat seizures and depression, respectively. However, it was discovered that these drugs also have pain-killing applications. Furthermore, since in cases of chronic or extreme pain, it is not unusual for an individual to suffer some degree of depression; antidepressants may serve a dual role. Commonly prescribed anticonvulsants for pain include phenytoin, carbamazepine, and clonazepam. Tricyclic antidepressants include doxepin, amitriptyline, and imipramine.
Intractable (unrelenting) pain may be treated by injections directly into or near the nerve that is transmitting the pain signal. These root blocks may also be useful in determining the site of pain generation. As the underlying mechanisms of abnormal pain are uncovered, other pain medications are being developed.
Drugs are not always effective in controlling pain. Surgical methods are used as a last resort if drugs and local anesthetics fail. The least destructive surgical procedure involves implanting a device that emits electrical signals. These signals disrupt the nerve and prevent it from transmitting the pain message. However, this method may not completely control pain and is not used frequently. Other surgical techniques involve destroying or severing the nerve, but the use of this technique is limited by side effects, including unpleasant numbness.
Alternative treatment
Both physical and psychological aspects of pain can be dealt with through alternative treatment. Some of the most popular treatment options include acupressure and acupuncture, massage, chiropractic, and relaxation techniques such as yoga, hypnosis, and meditation. Herbal therapies are gaining increased recognition as viable options; for example, capsaicin, the component that makes cayenne peppers spicy, is used in ointments to relieve the joint pain associated with arthritis. Contrast hydrotherapy can also be very beneficial for pain relief.
Lifestyles can be changed to incorporate a healthier diet and regular exercise. Regular exercise, aside from relieving stress, has been shown to increase endorphins, painkillers naturally produced in the body.
Prognosis
Successful pain treatment is highly dependent on successful resolution of the pain’s cause. Acute pain will stop when an injury heals or when an underlying problem is treated successfully. Chronic pain and abnormal pain are more difficult to treat, and it may take longer to find a successful resolution. Some pain is intractable and will require extreme measures for relief.
Prevention
Pain is generally preventable only to the degree that the cause of the pain is preventable. For example, improved surgical procedures, such as those done through a thin tube called a laparascope, minimize post-operative pain. Anesthesia techniques for surgeries also continuously improve. Some disease and injuries are often unavoidable. However, pain from some surgeries and other medical procedures and continuing pain are preventable through drug treatments and alternative therapies.
Resources
Periodicals
«Advances in Pain Management, New Focus Greatly Easing Postoperative Care.» Medical Devices & Surgical Technology Week September 26, 2004: 260.
Finn, Robert. «More than Half of Patients With Major Depression Have Chronic Pain.» Family Practice News October 15, 2004: 38.
«New Guidelines Set for Better Pain Treatment.» Medical Letter on the CDC & FDA September 5, 2004: 95.
Organizations
American Chronic Pain Association. P.O. Box 850, Rocklin, CA 95677-0850. (916) 632-0922. 〈http://members.tripod.com/∼widdy/ACPA.html〉.
American Pain Society. 4700 W. Lake Ave., Glenview, IL 60025. (847) 375-4715. http://www.ampainsoc.org.
Key terms
Acute pain — Pain in response to injury or another stimulus that resolves when the injury heals or the stimulus is removed.
Chronic pain — Pain that lasts beyond the term of an injury or painful stimulus. Can also refer to cancer pain, pain from a chronic or degenerative disease, and pain from an unidentified cause.
Neurotransmitters — Chemicals within the nervous system that transmit information from or between nerve cells.
Nociceptor — A neuron that is capable of sensing pain.
Referred pain — Pain felt at a site different from the location of the injured or diseased part of the body. Referred pain is due to the fact that nerve signals from several areas of the body may «feed» the same nerve pathway leading to the spinal cord and brain.
Stimulus — A factor capable of eliciting a response in a nerve.
Gale Encyclopedia of Medicine. Copyright 2008 The Gale Group, Inc. All rights reserved.
pain
[pān]
a feeling of distress, suffering, or agony, caused by stimulation of specialized nerve endings. Its purpose is chiefly protective; it acts as a warning that tissues are being damaged and induces the sufferer to remove or withdraw from the source. The North American Nursing Diagnosis Association has accepted pain as a nursing diagnosis, defining it as a state in which an individual experiences and reports severe discomfort or an uncomfortable sensation; the reporting of pain may be either by direct verbal communication or by encoded descriptors.
Pain Receptors and Stimuli. All receptors for pain stimuli are free nerve endings of groups of myelinated or unmyelinated neural fibers abundantly distributed in the superficial layers of the skin and in certain deeper tissues such as the periosteum, surfaces of the joints, arterial walls, and the falx and tentorium of the cranial cavity. The distribution of pain receptors in the gastrointestinal mucosa apparently is similar to that in the skin; thus, the mucosa is quite sensitive to irritation and other painful stimuli. Although the parenchyma of the liver and the alveoli of the lungs are almost entirely insensitive to pain, the liver and bile ducts are extremely sensitive, as are the bronchi and parietal pleura.
Some pain receptors are selective in their response to stimuli, but most are sensitive to more than one of the following types of excitation: (1) mechanical stress of trauma; (2) extremes of heat and cold; and (3) chemical substances, such as histamine, potassium ions, acids, prostaglandins, bradykinin, and acetylcholine. Pain receptors, unlike other sensory receptors in the body, do not adapt or become less sensitive to repeated stimulation. Under certain conditions the receptors become more sensitive over a period of time. This accounts for the fact that as long as a traumatic stimulus persists the person will continue to be aware that damage to the tissues is occurring.
The body is able to recognize tissue damage because when cells are destroyed they release the chemical substances previously mentioned. These substances can stimulate pain receptors or cause direct damage to the nerve endings themselves. A lack of oxygen supply to the tissues can also produce pain by causing the release of chemicals from ischemic tissue. Muscle spasm is another cause of pain, probably because it has the indirect effect of causing ischemia and stimulation of chemosensitive pain receptors.
Transmission and Recognition of Pain. When superficial pain receptors are excited the impulses are transmitted from these surface receptors to synapses in the gray matter (substantia gelatinosa) of the dorsal horns of the spinal cord. They then travel upward along the sensory pathways to the thalamus, which is the main sensory relay station of the brain. The dorsomedial nucleus of the thalamus projects to the prefrontal cortex of the brain. The conscious perception of pain probably takes place in the thalamus and lower centers; interpretation of the quality of pain is probably the role of the cerebral cortex.
The perception of pain by an individual is highly complex and individualized, and is subject to a variety of external and internal influences. The cerebral cortex is concerned with the appreciation of pain and its quality, location, type, and intensity; thus, an intact sensory cortex is essential to the perception of pain. In addition to neural influences that transmit and modulate sensory input, the perception of pain is affected by psychological and cultural responses to pain-related stimuli. A person can be unaware of pain at the time of an acute injury or other very stressful situation, when in a state of depression, or when experiencing an emotional crisis. Cultural influences also precondition the perception of and response to painful stimuli. The reaction to similar circumstances can range from complete stoicism to histrionic behavior.
Pain Control. There are several theories related to the physiologic control of pain but none has been completely verified. One of the best known is that of Mellzak and Wall, the gate control theory, which proposed that pain impulses were mediated in the substantia gelatinosa of the spinal cord with the dorsal horns acting as “gates” that controlled entry of pain signals into the central pain pathways. Also, pain signals would compete with tactile signals with the two constantly balanced against each other.
Since this theory was first proposed, researchers have shown that the neuronal circuitry it hypothesizes is not precisely correct. Nevertheless, there are internal systems that are now known to occur naturally in the body for controlling and mediating pain. One such system, the opioid system, involves the production of morphinelike substances called enkephalins and endorphins. Both are naturally occurring analgesics found in various parts of the brain and spinal cord that are concerned with pain perception and the transmission of pain signals. Signals arising from stimulation of neurons in the gray matter of the brain stem travel downward to the dorsal horns of the spinal cord where incoming pain impulses from the periphery terminate. The descending signals block or significantly reduce the transmission of pain signals upward along the spinal cord to the brain where pain is perceived by releasing these substances.
In addition to the brain’s opioid system for controlling the transmission of pain impulses along the spinal cord, there is another mechanism for the control of pain. The stimulation of large sensory fibers extending from the tactile receptors in the skin can suppress the transmission of pain signals from thinner nerve fibers. It is as if the nerve pathways to the brain can accommodate only one type of signal at a time, and when two kinds of impulses simultaneously arrive at the dorsal horns, the tactile sensation takes precedence over the sensation of pain.
The discovery of endorphins and the inhibition of pain transmission by tactile signals has provided a scientific explanation for the effectiveness of such techniques as relaxation, massage, application of liniments, and acupuncture in the control of pain and discomfort.
Assessment of Pain. Pain is a subjective phenomenon that is present when the person who is experiencing it says it is. The person reporting personal discomfort or pain is the most reliable source of information about its location, quality, intensity, onset, precipitating or aggravating factors, and measures that bring relief.
Objective signs of pain can help verify what a patient says about pain, but such data are not used to prove or disprove whether it is present. Physiologic signs of moderate and superficial pain are responses of the sympathetic nervous system. They include rapid, shallow, or guarded respiratory movements, pallor, diaphoresis, increased pulse rate, elevated blood pressure, dilated pupils, and tenseness of the skeletal muscles. Pain that is severe or located deep in body cavities acts as a stimulant to parasympathetic neurons and is evidenced by a drop in blood pressure, slowing of pulse, pallor, nausea and vomiting, weakness, and sometimes a loss of consciousness.
Behavioral signs of pain include crying, moaning, tossing about in bed, pacing the floor, lying quietly but tensely in one position, drawing the knees upward toward the abdomen, rubbing the painful part, and a pinched facial expression or grimacing. The person in pain also may have difficulty concentrating and remembering and may be totally self-centered and preoccupied with the pain.
Psychosocial aspects of tolerance for pain and reactions to it are less easily identifiable and more complex than physiologic responses. An individual’s reaction to pain is subject to a variety of psychologic and cultural influences. These include previous experience with pain, training in regard to how one should respond to pain and discomfort, state of health, and the presence of fatigue or physical weakness. One’s degree of attention to and distraction from painful stimuli can also affect one’s perception of the intensity of pain. A thorough assessment of pain takes into consideration all of these psychosocial factors.
Management of Pain. Among the measures employed to provide relief from pain, administration of analgesic drugs is probably the one that is most often misunderstood and abused. When an analgesic drug has been ordered “as needed,” the patient should know that the drug is truly available when needed and that it will be given promptly when asked for. If the patient is forced to wait until someone else decides when an analgesic is needed, the patient may become angry, resentful, and tense, thus diminishing or completely negating the desired effect of the drug. Studies have shown that when analgesics are left at the bedside of terminally ill cancer patients to be taken at their discretion, fewer doses are taken than when they must rely on someone else to make the drug available. Habituation and addiction to analgesics probably result as much from not using other measures along with analgesics for pain control as from giving prescribed analgesics when they are ordered. Patient-controlled analgesia has been used safely and effectively.
When analgesics are not appropriate or sufficient or when there is a real danger of addiction, there are noninvasive techniques that can be used as alternatives or adjuncts to analgesic therapy. The selection of a particular technique for the management of pain depends on the cause of the pain, its intensity and duration, whether it is acute or chronic, and whether the patient perceives the technique as effective.
Distraction techniques provide a kind of sensory shielding to make the person less aware of discomfort. Distraction can be effective in the relief of brief periods of acute pain, such as that associated with minor surgical procedures under local anesthesia, wound débridement, and venipuncture.
Massage and gentle pressure activate the thick-fiber impulses and produce a preponderance of tactile signals to compete with pain signals. It is interesting that stimulation of the large sensory fibers leading from superficial sensory receptors in the skin can relieve pain at a site distant from the area being rubbed or otherwise stimulated. Since ischemia and muscle spasm can both produce discomfort, massage to improve circulation and frequent repositioning of the body and limbs to avoid circulatory stasis and promote muscle relaxation can be effective in the prevention and management of pain. Transcutaneous electrical nerve stimulation (TENS) units enhance the production of endorphins and enkephalins and can also relieve pain.
Specific relaxation techniques can help relieve physical and mental tension and stress and reduce pain. They have been especially effective in mitigating discomfort during labor and delivery but can be used in a variety of situations. Learning proper relaxation techniques is not easy for some people, but once these techniques have been mastered they can be of great benefit in the management of chronic ongoing pain. The intensity of pain also can be reduced by stimulating the skin through applications of either heat or cold, menthol ointments, and liniments. Contralateral stimulation involves stimulating the skin in an area on the side opposite a painful region. Stimulation can be done by rubbing, massaging, or applying heat or cold.
Since pain is a symptom and therefore of value in diagnosis, it is important to keep accurate records of the observations of the patient having pain. These observations should include the following: the nature of the pain, that is, whether it is described by the patient as being sharp, dull, burning, aching, etc.; the location of the pain, if the patient is able to determine this; the time of onset and the duration, and whether or not certain nursing measures and drugs are successful in obtaining relief; and the relation to other circumstances, such as the position of the patient, occurrence before or after eating, and stimuli in the environment such as heat or cold that may trigger the onset of pain.
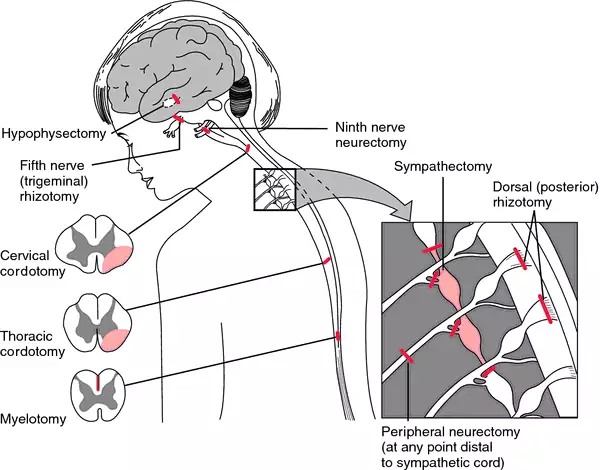
Surgical procedures designed to alleviate pain. From Ignatavicius et al., 1999.
acute pain
1. one of the three categories of pain established by the International Association for the Study of Pain, denoting pain that is caused by occurrences such as traumatic injury, surgical procedures, or medical disorders; clinical symptoms often include increased heart rate, blood pressure, and respiratory rate, shallow respiration, agitation or restlessness, facial grimaces, or splinting.
2. a nursing diagnosis accepted by the North American Nursing Diagnosis Association, defined as an unpleasant sensory and emotional experience arising from actual or potential tissue damage or described in terms of such damage, with sudden or slow onset of any intensity from mild to severe with an anticipated or predictable end and a duration of less than 6 months.
bearing-down pain pain accompanying uterine contractions during the second stage of labor.
cancer pain one of the three categories of pain established by the International Association for the Study of Pain, denoting pain associated with malignancies and perceived by the individual patient; there are various scales ranking it from 0 to 10 according to level of severity.
chronic pain
1. one of the three categories of pain established by the International Association for the Study of Pain, denoting pain that is persistent, often lasting more than six months; clinical symptoms may be the same as for acute pain, or there may be no symptoms evident. The North American Nursing Diagnosis Association has accepted chronic pain as a nursing diagnosis.
2. a nursing diagnosis accepted by the North American Nursing Diagnosis Association, defined as an unpleasant sensory and emotional experience arising from actual or potential tissue damage or described in terms of such damage, with sudden or slow onset of any intensity from mild to severe, without an anticipated or predictable end, and with a duration of greater than 6 months.
pain disorder a somatoform disorder characterized by a chief complaint of severe chronic pain that causes substantial distress or impairment in functioning; the pain is neither feigned nor intentionally produced, and psychological factors appear to play a major role in its onset, severity, exacerbation, or maintenance. The pain is related to psychological conflicts and is made worse by environmental stress; it enables the patient to avoid an unpleasant activity or to obtain support and sympathy. Patients may visit many health care providers searching for relief and may consume excessive amounts of analgesics without any effect. They are difficult to treat because they strongly resist the idea that their symptoms have a psychological origin.
false p’s ineffective pains during pregnancy that resemble labor pains, not accompanied by cervical dilatation; see also braxton-hicks contractions. Called also false labor.
growing p’s any of various types of recurrent limb pains resembling those of rheumatoid conditions, seen in early youth and formerly thought to be caused by the growing process.
hunger pain pain coming on at the time for feeling hunger for a meal; a symptom of gastric disorder.
intermenstrual pain pain accompanying ovulation, occurring during the period between the menses, usually about midway.
labor p’s the rhythmic pains of increasing severity and frequency due to contraction of the uterus at childbirth; see also labor.
lancinating pain sharp darting pain.
phantom pain pain felt as if it were arising in an absent or amputated limb or organ; see also amputation.
psychogenic pain symptoms of physical pain having psychological origin; see pain disorder.
referred pain pain in a part other than that in which the cause that produced it is situated. Referred pain usually originates in one of the visceral organs but is felt in the skin or sometimes in another area deep inside the body. Referred pain probably occurs because pain signals from the viscera travel along the same neural pathways used by pain signals from the skin. The person perceives the pain but interprets it as having originated in the skin rather than in a deep-seated visceral organ.
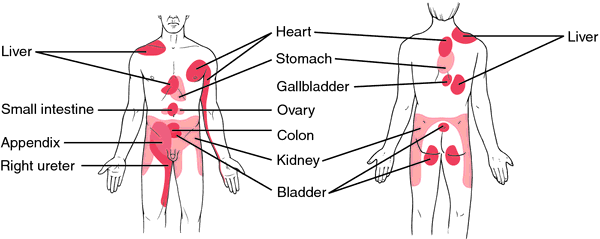
Area of referred pain, anterior and posterior views.
rest pain a continuous unrelenting pain due to ischemia of the lower leg, beginning with or being aggravated by elevation and being relieved by sitting with legs in a dependent position or by standing.
root pain pain caused by disease of the sensory nerve roots and occurring in the cutaneous areas supplied by the affected roots.
Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved.
pain
(pān),
1. A variably unpleasant sensation associated with actual or potential tissue damage and mediated by specific nerve fibers to the brain where its conscious appreciation may be modified by various factors.
2. Term used to denote a painful uterine contraction occurring in childbirth.
[L. poena, a fine, a penalty]
pain
algophobia.
Farlex Partner Medical Dictionary © Farlex 2012
pain
(pān)
n.
1. An unpleasant feeling occurring as a result of injury or disease, usually localized in some part of the body.
2. Mental or emotional suffering; distress.
3. One of the uterine contractions occurring in childbirth.
The American Heritage® Medical Dictionary Copyright © 2007, 2004 by Houghton Mifflin Company. Published by Houghton Mifflin Company. All rights reserved.
pain
Neurology ‘An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage’-per Intl Assn for Study of Pain; a sensation of discomfort, distress, or agony, due to stimulation of specialized nerve endings; a sensation of marked discomfort, either sharp and well-localized–conducted along A-delta fibers or dull and diffuse–conducted along C nerve fibers. See Acute pain, Acute low back pain, Ankle pain, Back pain, Breakthrough pain, Brief Pain Inventory, Central stroke pain, Chest pain, Chest wall pain, Chronic pain, Discogenic pain, Elbow pain, Gait control theory, Growing pain, Intractable pain, Knee pain, Lightning pain, Low back pain, Noncardiac chest pain, Patient controlled analgesia, Phantom limb pain, Substantial pain, Suprapubic pain.
McGraw-Hill Concise Dictionary of Modern Medicine. © 2002 by The McGraw-Hill Companies, Inc.
pain
(pān)
An unpleasant sensation associated with actual or potential tissue damage, and mediated by specific nerve fibers to the brain, where its conscious appreciation may be modified by various factors.
[L. poena, a fine, a penalty]
Medical Dictionary for the Health Professions and Nursing © Farlex 2012
pain
(pan) [Fr. peine, fr L. poena, a fine, a penalty, punishment]
As defined by the International Association for the Study of Pain, an unpleasant sensory and emotional experience arising from actual or potential tissue damage or described in terms of such damage. Pain includes not only the perception of an uncomfortable stimulus but also the response to that perception. About half of those who seek medical help do so because of the primary complaint of pain. Acute pain occurs with an injury or illness; is often accompanied by anxiety, diaphoresis, nausea, and vital sign changes such as tachycardia or hypertension; and should end after the noxious stimulus is removed or any organ damage heals. Chronic or persistent pain is discomfort that lasts beyond the normal healing period. Pain may arise in nearly any organ system and may have different characteristics in each. Musculoskeletal pain often is exacerbated by movement and may be accompanied by joint swelling or muscle spasm. Myofascial pain is marked by trigger-point tenderness. Visceral pain often is diffuse or vaguely localized, whereas pain from the lining of body cavities often is localized precisely, very intense, and exquisitely sensitive to palpation or movement. Neuropathic (nerve) pain usually stings or burns, or may be described as numbness, tingling, or shooting sensations. Colicky pain fluctuates in intensity from severe to mild, and usually occurs in waves. Referred pain results when an injury or disease occurs in one body part but is felt in another.
Several factors influence the experience of pain. Among these are the nature of the injury or illness causing the symptom, the physical and emotional health of the patient, the acuity or chronicity of the symptom, the social milieu and/or cultural upbringing of the patient, neurochemistry, memory, personality, and other features. See: table
Symptoms
Many clinicians use the mnemonic “COLDER” to aid the diagnosis of painful diseases. They will ask the patient to describe the Character, Onset, Location, and Duration of their painful symptoms, as well as the features that Exacerbate or Relieve it. For example: The pain of pleurisy typically is sharp in character, acute in onset, located along the chest wall, and long-lasting; it is worsened by deep breathing or coughing and relieved by analgesics or holding still. By contrast, the pain of myocardial ischemia usually is dull or heavy, gradual in onset, and located substernally. It may be worsened by activity (but not by taking a breath or coughing) and relieved by nitroglycerin.
In 2000, the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) issued pain-management standards, in 2001 began surveying for compliance, and in 2004 added patient-safety goals, thus most U.S. health care facilities have devised policies and procedures that require pain-intensity rating as a routine part of care (the fifth vital sign). Pain intensity usually is assessed on a numerical scale, in which 0 = no pain, 1 to 3 = mild pain, 4 to 6 = moderate pain, and 7 to 10 = severe pain. However, obtaining a numerical rating of pain intensity is possible only if the patient is able to provide this report of the pain being experienced, which infants, children, the critically ill, and cognitively impaired usually are unable to do. The Wong’ Baker FACES scale, developed for pediatric use, has been used successfully in other patient populations. It uses visual representations of smiles or grimaces to depict the level of pain a patient feels.
Patient care
Health care professionals must be aware that pain in non-verbal patient can easily be overlooked and must make a conscious effort to ensure that pain in these patients is assessed and treated. Observing subtle behaviors and being sensitive to contextual clues are two pain methods used by health care professionals to try to determine when nonverbal patients are in pain. When this judgment is made, a trial of pain-relieving medication may be used. The responses of the patient and any complications of treatment should be carefully observed and appropriate changes made in dosing or the type of analgesic drug as indicated.
Because pain is a subjective and intensely personal problem, sympathetic care is an important part of its relief. In addition to administering analgesic drugs, health care professionals should use a wide range of techniques to help alleviate pain, including local application of cold and heat, tactile stimulation, relaxation techniques, diversion, and active listening, among others.
acute pain
Pain that typically is produced by sudden injury (e.g., fracture) or illness (e.g., acute infection) and is accompanied by physical signs such as increased heart rate, elevated blood pressure, pupillary dilation, sweating, or hyperventilation. Acute pain is typically sharp in character. It is relayed to the central nervous system rapidly by A delta nerve fibers. [Then, at the end of this entry please add the SYN:] fast pain Depending on the severity of the underlying stimulus, acute pain may be managed with acetaminophen or anti-inflammatory drugs, immobilization and elevation of the injured body part, or the topical application of heat or ice. Severe acute pain, such as that of broken ribs or of an ischemic part, may require narcotics, often with adjunctive agents like hydroxyzine for relief, or antiemetics. Acute pain should be managed aggressively. Synonym: fast pain
adnexal pain
Discomfort arising from the fallopian tubes and ovaries; usually due to inflammation, infection, or ectopic pregnancy.
back pain
Pain felt in or along the spine or musculature of the posterior thorax. It is usually characterized by dull, continuous pain and tenderness in the muscles or their attachments in the lower lumbar, lumbosacral, or sacroiliac regions. Back pain is often referred to the leg or legs, following the distribution of the sciatic nerve.
Etiology
Common causes of back pain include pain caused by muscular or tendon strain, herniated intervertebral disk, lumbar spinal stenosis, or spondylolisthesis. Patients with a history of cancer may have back pain caused by metastatic tumors to the vertebrae and should be evaluated to be certain that damage to the spinal cord is not imminent. Patients with back pain and fever (esp. those with a history of injection drug use, tuberculosis, or recent back surgery) should be evaluated for epidural abscess or osteomyelitis.
Treatment
Depending on the underlying cause of the back pain, treatment may include drugs, rest, massage, physical therapy, chiropractic, stretching exercises, injection therapy, and surgery, among others. Most nonmalignant causes of back pain improve with a few days of rest, analgesics, and antiinflammatory drugs, followed by 2 to 4 weeks of anti-inflammatory treatment, appropriate muscle strengthening, and patience. Pain caused by an osteoporotic fracture may prove more debilitating and longer-lasting. Back pain produced by a spinal metastasis can improve with corticosteroids, radiation therapy, intravenous bisphosphonates, and/or surgical decompression. Patients with a spinal epidural abscess will need surgical drainage of the infection and antibiotics.
Patient care
Prolonged bedrest is inadvisable in most patients with back pain. The treatment regimen is explained, implemented, and reinforced. Factors that precipitate symptoms are identified and preventive actions are discussed.
bearing-down pains
Rectal pressure and discomfort occurring during the second stage of labor, related to fetal descent and the woman’s straining efforts to expel the fetus.
boring pain
Piercing, used to describe pain felt deep within the body.
breakthrough pain
Transient episodes of pain that occur in patients with chronic pain that has been previously reduced to tolerable levels. Breakthrough pain disrupts the well-being of cancer or hospice patients who have been prescribed regular doses of narcotic analgesics. The painful episodes may occur as a previous dose of pain-relieving medication wears off (“end-of-dose pain”), or after unusual or unanticipated body movements (“incident pain”).
Brodie pain
Pain caused near a joint affected with neuralgia when the skin is folded near it.
burning pain
Pain experienced in heat burns, superficial skin lesions, herpes zoster, and circumscribed neuralgias.
causalgic pain
Causalgia.
central pain
Pain due to a lesion in the central nervous system.
chest pain
Discomfort felt in the upper abdomen, thorax, neck, or shoulders. Chest pain is one of the most common potentially serious complaints offered by patients in emergency departments, hospitals, outpatient settings, and physicians’ offices. A broad array of diseases and conditions may cause it, including (but not limited to) angina pectoris or myocardial infarction; anxiety and hyperventilation; aortic dissection; costochondritis or injured ribs; cough, pneumonia, pleurisy, pneumothorax, or pulmonary emboli; esophageal diseases, such as reflux or esophagitis; gastritis, duodenitis, or peptic ulcer; and stones in the biliary tree.
chronic idiopathic pelvic pain
Abbreviation: CIPP
Unexplained pelvic pain in a woman that has lasted 6 months or longer. A complete medical, social, and sexual history must be obtained. In an experimental study, women with this illness reported more sexual partners, significantly more spontaneous abortions, and previous nongynecological surgery. These women were more likely to have experienced previous significant psychosexual trauma.
Treatment
The pain associated with CIPP should be treated symptomatically and sympathetically. The participation of pain management specialists, complementary medical providers, and the primary health care provider should be integrated. Realistic goals (e.g., the reduction of pain rather than its elimination) should be set. Medroxyprogesterone acetate, oral contraceptives, presacral neurectomy, hypnosis, and hysterectomy have been tried with varying degrees of success.
chronic pain
1. Long-lasting discomfort, with episodic exacerbations, that may be felt in the back, one or more joints, the pelvis, or other parts of the body.
2. Pain that lasts more than 3–6 months.
3. Pain that lasts more than a month longer than the usual or expected course of an illness.
4. Pain that returns periodically every few weeks or months for many years. Chronic pain is often described by sufferers as being debilitating, intolerable, disabling, or alienating and may occur without an easily identifiable cause. Studies have shown a high correlation between chronic pain and depression or dysphoria, but it is unclear whether the psychological aspects of chronic pain precede or develop as a result of a person’s subjective suffering. Chronic pain is the leading cause of disability in the U.S.acute pain;
Patient care
The management of chronic, nonmalignant pain is often difficult and may be frustrating for both sufferer and caregiver. The best results are usually obtained through multimodal therapy that combines sympathetic guidance that encourages patients to recover functional abilities, by combinations of drugs (e.g., nonsteroidal anti-inflammatories, narcotic analgesics, and/or antidepressants), physical therapy and regular exercise, occupational therapy, physiatry, psychological or social counseling, and alternative medical therapies (e.g., acupuncture, massage, or relaxation techniques). Placebos, although rarely employed clinically, effectively treat chronic pain in about a third of all patients. Surgery and other invasive strategies are occasionally employed, with variable effectiveness.
cramplike pain
Cramp.
dental pain
Pain in the oral area, which, in general, may be of two origins. Soft tissue pain may be acute or chronic, and a burning pain is due to surface lesions and usually can be discretely localized; pulpal pain or tooth pain varies according to whether it is acute or chronic, but it is often difficult to localize.
dilating pain
Discomfort accompanying rhythmic uterine contractions during the first stage of labor.
diskogenic pain
Low back pain resulting from degeneration of an intervertebral disk. Discogenic pain differs from neuropathic pain in that it does not radiate into the extremities or torso.
dull pain
A mild discomfort, often difficult to describe, that may be associated with some musculoskeletal injuries or some diseases of the visceral organs.
eccentric pain
Pain occurring in peripheral structures owing to a lesion involving the posterior roots of the spinal nerves.
epigastric pain
Pain located between the xiphoid process and the umbilicus. It may suggest a problem in one of many different organs, including the stomach, pancreas, gallbladder, small or large bowel, pleura, or heart.
Synonym: gastralgic pain See: cardialgia
expulsive pains
Discomfort during the second stage of labor, associated with bearing-down efforts to expel the fetus. Women may experience a similar pain during delivery of the placenta.
false pain
Abdominal discomfort associated with Braxton Hicks contractions, which occur during the last trimester of pregnancy. Characteristically, the woman complains of irregular, lower abdominal pains, which are relieved by walking. Vaginal examination shows no change in cervical effacement or dilation.
See: Braxton Hicks contractions
fast pain
Acute pain.
fulgurant pain
Lightning pain.
gallbladder pain
Biliary colic.
gas pain
Pain in the intestines caused by an accumulation of gas therein.
gastralgic pain
Epigastric pain.
girdle pain
Zonesthesia.
growing pains
An imprecise term indicating ill-defined pain, usually in the shin or other areas of the legs, typically occurring after bedtime in children age 5 to 12. There is no evidence that the pain is related to rapid growth or to emotional problems. If these symptoms occur during the daytime, are accompanied by other symptoms, or become progressively more severe, evaluation for infection, cancer, and other diseases of muscle and bone should be undertaken. In the majority of cases, this evaluation is not necessary.
Treatment
The child should be reassured and given acetaminophen or ibuprofen; heat and massage can be applied locally. Children with growing pains benefit from concern and reassurance from their parents and health care providers.
heterotopic pain
Referred pain.
homotopic pain
Pain felt at the point of injury.
hunger pain
Pain in the epigastrum that occurs before meals.
incident pain
Pain due to a sudden, forceful, unanticipated, or unusual body movement or posture.
inflammatory pain
Pain in the presence of inflammation that is increased by pressure.
intermenstrual pain
Episodic, localized pelvic discomfort that occurs between menstrual periods, possibly accompanying ovulation.
Synonym: midpain See: mittelschmerz
intractable pain
Chronic pain that is difficult or impossible to manage with standard interventions. Common causes include metastatic cancer, chronic pancreatitis, radiculopathy, spinal cord transection, or peripheral neuropathy. Intractable pain may also accompany somatoform disorders, depression, fibromyalgia, irritable bowel syndrome, and opiate dependence. Various combinations of the following management strategies are often used to treat intractable pain: antidepressant medications, counseling, deep brain stimulation, injected anesthetics, narcotic analgesics, neurological surgery, and pain clinic consultations.
labor pains
Uncomfortable, intermittent, rhythmic, girdling sensations associated with uterine contractions during childbearing. The frequency, duration, and intensity of the events increase, climaxing with the delivery of the fetus.
lancinating pain
Acute pain.
lightning pain
A sudden brief pain that may be repetitive, usually in the legs but may be at any location. It is associated with tabes dorsalis and other neurological disorders. Synonym: fulgurant pain
lingual pain
Pain in the tongue that may be due to local lesions, glossitis, fissures, or pernicious anemia. Synonym: tongue pain
lung pain
Sharp pain in the region of the lungs.
menstrual pain
Dysmenorrhea.
mental pain
Psychogenic pain.
middle pain
Intermenstrual pain.
mobile pain
Pain that moves from one area to another.
movement pain
Kinesalgia.
neuropathic pain
Pain that originates in peripheral nerves or the central nervous system rather than in other damaged organs or tissues. A hallmark of neuropathic pain is its localization to specific dermatomes or nerve distributions. Some examples of neuropathic pain are the pain of shingles (herpes zoster), diabetic neuropathy, radiculopathy, and phantom limb pain.
Treatment
Drugs like gabapentin or pregabalin provide effective relief of neuropathic pain for some patients. Other treatments include (but are not limited to) regional nerve blocks, selective serotonin and norepinephrine reuptake inhibitors, psychological counseling, acupuncture, transcutaneous electrical nerve stimulation, and physical therapy.
night pain
Pain that awakens the patient at night or interferes with sleep; may be due to infection, inflammation, neurovascular compromise, or severe structural damage.
noise pain
Odynacusis.
objective pain
Pain induced by some external or internal irritant, by inflammation, or by injury to nerves, organs, or other tissues that interferes with the function, nutrition, or circulation of the affected part. It is usually traceable to a definite pathologic process.
paresthesic pain
A stinging or tingling sensation manifested in central and peripheral nerve lesions.
See: paresthesia
periodontal pain
A discrete, well-localized pain caused by inflammation of tissues surrounding a tooth. This may be contrasted with the throbbing, nonlocalized pain typical of a toothache or pulpal pain.
phantom limb pain
The sensation of pain felt in the nerve distribution of a body part that has been amputated. Phantom pain can lead to difficulties in prosthetic training. Synonym: phantom sensation
Patient care
Phantom limb pain or nonpainful sensations are reported by most amputees. A multimodal or combination approach to management is appropriate. Drugs used to treat neuropathic pain may be helpful, including some anticonvulsant drugs, tricyclic antidepressants, selective serotonin inhibitors, and muscle relaxants. Nerve blockade and/or transcutaneous electrical stimulation may also be helpful. Health care professionals should encourage amputees to move the affected extremity, seek counseling or group therapy, engage in physical and occupational therapy, and use distraction techniques.
postprandial pain
Abdominal pain after eating.
precordial pain
Pain felt in the center of the chest (e.g., below the sternum) or in the left side of the chest.
premonitory pain
Ineffective contractions of the uterus before the beginning of true labor.
See: false pain
pseudomyelic pain
The false sensation of movement in a paralyzed limb or of no movement in a moving limb; not a true pain.
psychogenic pain
Pain having mental, as opposed to organic, origin.
radicular pain
Pain that radiates away from the spinal column through an extremity or the torso resulting from the compression or irritation of a spinal nerve root or large paraspinal nerve. It may be accompanied by numbness or tingling.
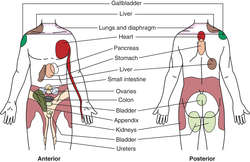
![]()
SITES OF REFERRED PAIN
referred pain
Pain that arises in one body part or location but is perceived in another. For example, pain caused by inflammation of the diaphragm often is felt in the shoulder; pain caused by myocardial ischemia may be referred to the neck or jaw; and pain caused by appendicitis may first be felt near the umbilicus rather than in the right lower quadrant, where the appendix lies. See: table
Synonym: heterotopic pain; sympathetic pain See: illustration
remittent pain
Pain with temporary abatements in severity; characteristic of neuralgia and colic.
rest pain
Pain due to ischemia that comes on when sitting or lying.
root pain
Cutaneous pain caused by disease of the sensory nerve roots.
shooting pain
Pain that seems to travel like lightning from one place to another.
slow pain
Pain that is perceived a second or more after a stimulus. It is transmitted to the central nervous system by C (nerve) fibers, which are not myelinated, and therefore conduct sensations more slowly than A delta fibers. Slow pain lasts longer than sudden pain. It is usually perceived by patients as burning, cramping, dull, itchy, or warm.
standards for pain relief
Standards for the Relief of Acute Pain and Cancer Pain developed by the American Pain Society. These are summarized as follows:
1. In order to increase the clinician’s responsiveness to complaints of pain, it is now considered by some health care professionals to be the fifth vital sign.2. Acute pain and cancer pain are recognized and effectively treated. Essential to this process is the development of a clinically useful and easy-to-use scale for rating pain and its relief. Patients will be evaluated according to the scales and the results recorded as frequently as needed.3. Information about analgesics is readily available. This includes data concerning the effectiveness of various agents in controlling pain and the availability of equianalgesic charts wherever drugs are used for pain.4. Patients are informed on admission of the availability of methods of relieving pain, and that they must communicate the presence and persistence of pain to the health care staff.5. Explicit policies for use of advanced analgesic technologies are defined. These advances include patient-controlled analgesia, epidural analgesia, and regional analgesia. Specific instructions concerning use of these techniques must be available for the health care staff.6. Adherence to standards is monitored by an interdisciplinary committee. The committee is responsible for overseeing the activities related to implementing and evaluating the effectiveness of these pain standards.
starting pain
A pain accompanied by muscular spasm during the early stages of sleep.
subdiaphragmatic pain
A sharp stitchlike pain occurring during breathing caused, for example, by an abscess or tumor beneath the diaphragm. When the breath is held, the pain ceases. Pressure against the lower rib cage eases the pain.
subjective pain
Psychogenic pain.
sympathetic pain
Referred pain.
tenesmic pain
Tenesmus.
terebrant pain
A boring or piercing type of pain.
thalamic pain
See: thalamic syndrome
thermalgesic pain
Pain caused by heat.
thoracic pain
Chest pain.
throbbing pain
Pain found in dental caries, headache, and localized inflammation. The pain is often thought to be caused by arterial pulsations.
tongue pain
Lingual pain.
tracheal pain
Trachealgia.
vascular pain
Pain that throbs or pulses, such as the pain of a migraine headache.
wandering pain
Pain that changes its location repeatedly.
Harrison’s Principles of Internal Medicine,
| Nonopioid Analgesics | |||
|---|---|---|---|
| Generic Name | Dose, mg * | Interval | Comments |
| Acetylsalicylic acid | 325–650 | 4–24 hr | Enteric-coated preparations available |
| Acetaminophen | 650 | 4 hr | Avoid in liver failure |
| Ibuprofen | 400–800 | 4–8 hr | Available without prescription |
| Indomethacin | 25–75 | 8 hr | Gastrointestinal and kidney side effects common |
| Naproxen | 250–500 | 12 hr | Delayed effects may be due to long half-life |
| Ketorolac | 15–60 IM | 4–6 hr | Similar to ibuprofen but more potent |
| Opioid Analgesics | |||
| Generic Name | Parenteral Dose (mg) | PO Dose (mg) | Comments |
| Codeine | 30–60 every 4 hr | 30–60 every 4 hr | Nausea common |
| Hydromorphone | 1–2 every 4 hr | 2–4 every 4 hr | Shorter acting than morphine sulfate |
| Levorphanol | 2 every 6–8 hr | 4 every 6 hr | Longer acting than morphine sulfate; absorbed well PO |
| Methadone | 10–100 | 6–24 hr | Delayed sedation due to long half-life |
| Meperidine | 25–100 | 300 every 4 hr | Poorly absorbed PO; normeperidine is a toxic metabolite |
| Morphine | 10 every 4 hr | 60 every 4 hr | |
| Morphine, sustained release | 30–90 | 60–180 2 or 3 times daily | |
| Oxycodone | — | 5–10 every 4–6 hr | Usually available with acetaminophen or aspirin |
* By mouth unless indicated otherwise.PO—by mouth only.SOURCE: Adapted from Isselbacher, K.J., et al.: ed 13. McGraw-Hill, New York, 1994.NOTE: L = left; R = right.
| Organ of Origin | Location Felt |
|---|---|
| Head | External or middle ear |
| Nose & sinuses | |
| Teeth, gums, tongue | |
| Throat, tonsils | |
| Parotid gland, TMJ joint | |
| Thorax | |
| Diaphragm | Shoulder, upper abdomen |
| Heart | Upper chest, L shoulder, inside L arm, L jaw |
| Abdomen | |
| Stomach & spleen | L upper abdomen |
| Duodenum | Upper abdomen, R shoulder |
| Stomach & spleen | L upper abdomen |
| Stomach & spleen | L upper abdomen |
| Stomach & spleen | L upper abdomen |
| Colon | Lower abdomen |
| Appendix | Periumbilical and R lower abdomen |
| Pelvis | |
| Appendix | Periumbilical and R lower abdomen |
Medical Dictionary, © 2009 Farlex and Partners
pain
An unpleasant or distressing localized sensation caused by stimulation of certain sensory nerve endings called nociceptors, or by strong stimulation of other sensory nerves. Nociceptors are stimulated by the chemical action of substances, such as prostaglandins, released from local cell damaged by injury or inflammation. Whatever the site of nerve stimulation, pain is usually experienced in the region of the nerve endings. Referred pain is pain experienced at a site other than that at which the causal factor is operating. Pain impulses pass to the brain via a series of control ‘gates’ analogous to those in computers and these can be modulated by other nerve impulses. Pain commonly serves as a warning of bodily danger and leads to action to end it. Pain is best treated by discovering and removing the cause. It is a complex phenomenon with many components-somatic, emotional, cognitive and social. The management of acute, self-limiting pain is not the same as long-term pain. The latter requires treatment by a multidisciplinary team in a pain clinic. ANALGESIC drugs can be used to target specific receptors and should not be withheld until pain is severe but given repeatedly in expectation of pain. Pain may be relieved by drugs self-administered on an as-required basis; by electrical stimulation of the skin; ACUPUNCTURE; massage; cold sprays; LOCAL ANAESTHETIC injections; or even, in extreme cases and rarely, by permanent nerve destruction by alcohol injection or by surgical severance. From the Latin poena, punishment. See also ENDORPHINS.
Collins Dictionary of Medicine © Robert M. Youngson 2004, 2005
pain
an unpleasant, conscious sensation produced in the brain and stimulated by pain receptors in, for example, the skin. Pain has a protective function and often produces a reflex action (see REFLEX ARC in response.
Collins Dictionary of Biology, 3rd ed. © W. G. Hale, V. A. Saunders, J. P. Margham 2005
pain
(pān)
Variably unpleasant sensation associated with tissue damage and mediated by specific nerve fibers to brain where its conscious appreciation is modified.
[L. poena, a fine, a penalty]
Medical Dictionary for the Dental Professions © Farlex 2012
Patient discussion about pain
Q. Pulling pain in anus. Dear friends, I am 32. I feel a Pulling pain in anus sometimes while i finish passing stool and some times when i sit for long time. No bleeding so far. Is it a symptoms of piles? If so what can be done to cure it without going to doctor or operation. Please help me. This pain makes me to feel that i am very old.
A. horsechestnut is supposed to help…here is some info about it:
http://nccam.nih.gov/health/horsechestnut/index.htm#uses
but i wouldn’t get my hopes high.
Q. Polio Syndrome pain One of my aunt is taking Neurontin for Post Polio Syndrome pain in her left leg and arm. she did not realize that she had so much pain and that it was keeping her from doing so many things. Is Neurontin recomended for this treatment and how does it help? Will she have problems with Neurontin if she take it long term? Neurontin is greatly helping the pain but not the fatique in these limbs. Should it help the fatigue?
A. Neurontin is being given as medication for nerve pain now also…I take 800 mg a day and it was started for back pain and it is also being used in some fibro patients I am learning( i also have fibromyalgia) It didn’t cause me a lot of drowsness but amount of medication and medications affect people differently so each person can be different. But with the fatigue fibromyalgia causes maybe I just can’t tell the difference b/c before I started it I was tried all the time and that is not any worse. But if your Aunt and yourself feel uncomfortable with this treatment I would suggest a second opinion. Good Luck to your Aunt
Q. Why do they think that the pain is all in my head? Is there any chance which may wrongfully lead doctor to conclude that our symptoms are of a psychological nature? Why do they think that the pain is all in my head?
A. It may happen very rarely and if he is new to his profession. It doesn’t mean that all those are new to their profession does these mistakes. Doctors cannot «see» and may not understand the sources of your pain or fatigue. However, what they do observe is your anxiety and frustration with having to deal with these symptoms around-the-clock, which may wrongfully lead them to conclude that your symptoms are of a psychological nature. Also, the old school of thought regarding pain is that it is produced by tissue injury, and there is no obvious source of tissue injury in patients with fibromyalgia. Regardless, if your doctor does not believe that your symptoms are real, you owe it to yourself to find another doctor who believes in you and will work with you to help reduce your symptoms.
More discussions about pain
This content is provided by iMedix and is subject to iMedix Terms. The Questions and Answers are not endorsed or recommended and are made available by patients, not doctors.
The work of the Task Force on Taxonomy in the era of 1979 to 1994 has been continued by the Committee on Taxonomy that has worked to update both pain terms and the classification of pain syndromes. All of the terms have been carefully reviewed and their utility assessed in reference to new knowledge about both clinical and basic science aspects of pain. The Committee conducted its business primarily by e-mail, but face-to-face meetings were held at each of the annual Congresses of IASP. We now present the 2011 version of IASP Pain Terminology. Members of the Taxonomy Committee in this era included: David Boyd, Michael Butler, Daniel Carr, Milton Cohen, Marshall Devor, Robert Dworkin, Joel Greenspan, Troels Jensen, Steven King, Martin Koltzenburg, John Loeser, Harold Merskey, Akiko Okifuji, Judy Paice, Jordi Serra, Rolf-Detlef Treede, and Alain Woda. The Chair would like to acknowledge the continuous contributions that Harold Merskey has made to taxonomy since the founding of IASP. As stated in prior publications of the IASP taxonomy, we do not see this listing of terms as immutable. As we learn more about pain, we will need to update terminology.
John D. Loeser, M.D.
Chair, IASP Terminology Working Group
Рассказали, какие существительные, глаголы и прилагательные подходят для описания физической боли.
С болью мы сталкиваемся постоянно: от ломоты в теле при простуде до горящих ног после долгой прогулки, от прострела в пояснице до пульсации в висках. Сегодня научимся описывать свои ощущения на английском.
Какими синонимами заменить pain и ache
Уверены, что вам знакомы существительные (a) pain и an ache, которые переводятся как «боль». (A) pain используется для описания боли любой интенсивности в любой части тела. An ache означает продолжительную тупую боль и чаще употребляется в таких сочетаниях, как (a) tummy ache (боль в животе или желудке), (a) backache (боль в спине), (a) toothache (зубная боль), (a) headache (головная боль), (an) earache (боль в ушах).
Did he explain what might have caused the pain in your knee? — Он объяснил, что могло вызвать эту боль в колене?
I’ve bought some medicine for your earache. I hope it helps. — Я купила лекарство от твоей боли в ушах. Надеюсь, поможет.
Когда вы говорите о незначительных болях, не уточняя в какой части тела, используйте фразу aches and pains (незначительная боль).
I usually take paracetamol to ease aches and pains. — При незначительных болях я обычно пью парацетамол.
А теперь рассмотрим слова, которые помогут точнее описать характер болезненных ощущений.
| Слово | Пример |
|---|---|
| agony — мучительная боль | Everyone who has ever broken their leg understands what agony means. — Каждый, кто ломал ногу, понимает, что такое мучительная боль. |
| soreness — боль, болезненные ощущения (обычно вызванные инфекцией или чрезмерными нагрузками) | My mum has been using a special ointment to reduce soreness in her shoulders. — Мама пользуется специальной мазью, чтобы уменьшить болезненные ощущения в плечах. |
| discomfort — недомогание, дискомфорт | The operation was successful, but I experienced some slight discomfort for the following three weeks. — Операция прошла успешно, но последующие три недели я ощущала легкий дискомфорт. |
| a pang — внезапная резкая боль, спазм, приступ боли | They hadn’t eaten since early morning and the hunger pangs were getting more and more intense. — Они не ели с раннего утра, и голодные спазмы становились все сильнее. |
| a prick — укол | I felt a prick in my arm but didn’t pay much attention to it. — Я почувствовал, как что-то кольнуло в руке, но не придал этому особого значения. |
| a sting — чувство жжения | I felt a terrible sting as some salt got in the cut on my hand. — Я почувствовала ужасное жжение, когда соль попала на порез на руке. |
| a twinge — резкая боль | I get twinges in my lower back now and again. — Время от времени у меня в пояснице появляются резкие боли. |
| (a) cramp — спазм, судорога | A cramp in her right leg didn’t let her continue the race. — Судорога в правой ноге не позволила ей продолжить гонку. |
| a throb — пульсирующая боль | I felt a strange throb behind my right eye. — Я почувствовала странную пульсирующую боль под правым глазом. |
| colic — резь, колики | Colic is a common problem faced by new parents. — Колики — частая проблема, с которой сталкиваются молодые родители. |
| (a) stitch — колющая боль в боку | I got a stitch after trying to catch up with the dog. — У меня появилась колющая боль в боку, после того как я попыталась догнать собаку. |
It hurts: как описать виды боли
Чтобы описать внезапную острую боль или продолжительные болезненные ощущения, носитель чаще всего использует глагол to hurt (болеть, мучить).
It hurts when I move my big toe. — Мне больно, когда я шевелю большим пальцем.
My neck is really hurting me today. — У меня сегодня ужасно болит шея.
Чтобы разнообразить речь, заменяйте глагол to hurt более точными синонимами:
| Слово/Выражение | Пример |
|---|---|
| to ache — болеть, ныть | Are your legs still aching from our run yesterday? — У тебя все еще болят ноги после нашей вчерашней пробежки? |
| to trouble, to bother — беспокоить | The ulcer had been troubling my father for two years before he finally went to the doctor’s. — Язва беспокоила моего отца два года, пока он наконец не пошел к врачу. |
| to be killing smb (informal) — мучить, добивать | I’ve been sleeping in an awkward position, and now my neck is killing me. — Я спала в неудобном положении, и теперь меня мучит шея. |
| to act up, to play up (informal) — болеть, разболеться, разыграться | My left ankle, which I sprained half a year ago, has been playing up again. — У меня снова разболелась левая лодыжка, которую я подвернула полгода назад. |
| to give smb grief (informal) — мучить, не давать покоя | My boyfriend is going to the dentist again. His teeth are giving him grief. — Мой парень снова идет к стоматологу. Зубы не дают ему покоя. |
| to sting — колоть, жечь | His skin stung from the new aftershave his wife had bought him. — Он ощутил жжение на коже от нового геля после бритья, который ему подарила жена. |
| to smart — болеть, щипать | The smoke in the kitchen made her eyes smart. — От дыма на кухне у нее защипало в глазах. |
| to burn — жечь | The student’s eyes were burning from the chemicals he was working with. — От химикатов, с которыми работал студент, у него жгло в глазах. |
| to pinch — давить | The turtleneck is too tight, it is pinching my neck. — Водолазка слишком тесная, она сдавливает горло. |
| to throb — пульсировать | Her feet were throbbing after the tiring hike in the mountains. — После утомительного похода в горы у нее пульсировало в ногах. |
Помимо глаголов, рассказать о боли помогут и прилагательные bad (больной) и sore (больной, воспаленный, болит).
If she hadn’t drunk so much yesterday, she wouldn’t have got a bad head in the morning. — Если бы она вчера столько не пила, то утром у нее бы не болела голова.
I can’t sing when I have a sore throat. — Я не могу петь, когда у меня болит горло.
Как рассказать о характере болевых ощущений
Само по себе слово (a) pain не дает информации о характере боли, поэтому нередко используется с уточняющими прилагательными.
Грамотно сказать о том, как часто появляются боли, помогут прилагательные chronic (хроническая), constant/persistent (постоянная), continuous (продолжительная) и intermittent (периодическая).
Is it possible to get rid of chronic back pain once and for all? — Возможно ли избавиться от хронической боли в спине раз и навсегда?
Continuous pains in his knees doesn’t let him fully enjoy his life. — Постоянные боли в коленях не дают ему в полной мере наслаждаться жизнью.
She’s been having intermittent pains in her stomach for around two months. — У нее уже около двух месяцев появляются периодические боли в желудке.
Рассказать об интенсивности болевых ощущений вам помогут прилагательные из таблицы.
| Слово | Пример |
|---|---|
| unbearable — невыносимая, нестерпимая | The man was taken to hospital complaining of unbearable abdominal pain. — Мужчину положили в больницу с жалобами на невыносимую боль в животе. |
| agonizing, excruciating — мучительная | He felt an excruciating pain in his side and gritted his teeth. — Он почувствовал мучительную боль в боку и стиснул зубы. |
| severe, intense, extreme — сильная, острая | Excessive physical exercise can cause intense muscle pain. — Чрезмерные физические нагрузки могут вызвать сильную боль в мышцах. |
| sharp, acute — острая | She winced as a sharp pain shot up her shoulder. — Она вздрогнула, когда острая боль пронзила ее плечо. |
| awful, terrible — ужасная | As he hit his little toe on the bed, he felt an awful pain. — Ударившись мизинцем об кровать, он почувствовал ужасную боль. |
| moderate — умеренная | Moderate pain can grow stronger if you don’t do anything for it. — Умеренная боль может усилиться, если ты ничего не предпримешь. |
| mild, slight — слабая | I occasionally have slight pains in my left wrist. — Иногда у меня появляются слабые боли в левом запястье. |
«Можете описать свою боль? Стреляющая, давящая, ноющая?» — такие вопросы от врачей не редкость, поэтому следует научиться отвечать на них по-английски.
| Слово | Пример |
|---|---|
| burning — жгучая | After painting the walls for five hours I started to feel a burning pain in my eyes. — После того как я пять часов красила стены, я начала чувствовать жгучую боль в глазах. |
| dull — тупая | Despite the dull pain in his shin, he carried on running. — Несмотря на тупую боль в голени, он продолжил бежать. |
| stinging — жгучая, жалящая | I realized that I had been bitten by a spider only when I felt a stinging pain in my arm. — Я поняла, что меня укусил паук, только когда почувствовала жгучую боль в руке. |
| searing — раздирающая | I took a painkiller to dull the searing pain in my leg. — Я выпила обезболивающее, чтобы притупить раздирающую боль в ноге. |
| shooting — стреляющая, дергающая | Shooting pains in the lower back can be lessened by deep massage. — Стреляющие боли в пояснице можно облегчить с помощью глубокого массажа. |
| stabbing — колющая, режущая | I couldn’t concentrate on my work because of a stabbing pain in my neck. — Я не могла сосредоточиться на работе из-за режущей боли в шее. |
| gnawing — ноющая, грызущая | Some people don’t think gnawing pains in the joints are anything to worry about. — Некоторые люди считают, что ноющие боли в суставах не повод волноваться. |
| nagging — ноющая, тянущая | This ointment might help to ease your nagging back pain. — Эта мазь может помочь тебе облегчить тянущую боль в спине. |
| boring — сверлящая | A boring pain in the back of the head kept me awake all night. — Сверлящая боль в затылке не давала мне спать всю ночь. |
| crushing — сжимающая, давящая | I felt a crushing pain in my stomach and called an ambulance. — Я почувствовала давящую боль в животе и вызвала скорую. |
| gripping — сжимающая | You may experience some gripping pain, but it will wear off in a few minutes. — Вы можете почувствовать сжимающую боль, но через несколько минут она пройдет. |
| throbbing — пульсирующая | I’ve been having a throbbing pain in the temples for about a week. — Меня уже неделю мучает пульсирующая боль в висках. |
Обратите внимание, что слова splitting (сильная, раскалывающая) и thumping/pounding (сильная, пульсирующая) используются только при описании головной боли:
I wish I could come to your party, but I’ve got a splitting headache today. — Я бы рада прийти на твою вечеринку, но у меня голова сегодня раскалывается.
I woke up with a thumping headache. — Я проснулась с сильной головной болью.
What can be worse than a pounding headache getting in the way of your day? — Что может быть хуже, чем пульсирующая головная боль, которая портит весь день?
Мы рассмотрели лексику для описания боли, и теперь вам не составит труда рассказать врачу или пожаловаться другу о своих проблемах. Больше выражений вы найдете в статьях «Разница между ache, pain, hurt, sick и ill» и «Как вести диалог у врача в больнице на английском языке: удобный разговорник». Берегите себя и будьте здоровы!
Предлагаем пройти небольшой тест и проверить, что вы запомнили.
Тест по теме «Aches and pains: описываем боль по-английски»
© 2023 englex.ru, копирование материалов возможно только при указании прямой активной ссылки на первоисточник.
ФГАОУ ВО «Первый Московский государственный медицинский университет им. И.М. Сеченова» Минздрава России (Сеченовский Университет)
- SPIN РИНЦ: 6438-3370
- Scopus AuthorID:
7004210424 - ORCID:
0000-0002-8255-5645
Кукушкин М.Л.
ФГБНУ «Научно-исследовательский институт общей патологии и патофизиологии»
Чурюканов М.В.
ФГАОУ ВО «Первый Московский государственный медицинский университет им. И.М. Сеченова» Минздрава России (Сеченовский университет);
ФГБНУ «Российский научный центр хирургии им. акад. Б.В. Петровского» Минобрнауки России
Давыдов О.С.
ФГБНУ «Научно-исследовательский институт общей патологии и патофизиологии» Минобрнауки России
Бахтадзе М.А.
ФГАОУ ВО «Российский национальный исследовательский медицинский университет им. Н.И. Пирогова» Минздрава России;
ГБУЗ Москвы «Центр мануальной терапии Департамента здравоохранения Москвы»

Новое определение боли Международной ассоциации по изучению боли
Авторы:
Яхно Н.Н., Кукушкин М.Л., Чурюканов М.В., Давыдов О.С., Бахтадзе М.А.
Как цитировать:
Яхно Н.Н., Кукушкин М.Л., Чурюканов М.В., Давыдов О.С., Бахтадзе М.А. Новое определение боли Международной ассоциации по изучению боли. Российский журнал боли.
2020;18(4):5‑7.
Yakhno NN, Kukushkin ML, Churyukanov MV, Davydov OS, Bakhtadze MA. New definition of pain by the international association for the study of pain. Russian Journal of Pain. 2020;18(4):5‑7. (In Russ.)
https://doi.org/10.17116/pain2020180415
Определение боли Международной ассоциации по изучению боли (IASP) как «неприятное сенсорное и эмоциональное переживание, связанное с действительным или возможным повреждением тканей или описываемое в терминах такого повреждения» было рекомендовано подкомитетом по таксономии и принято Советом IASP в 1979 г. [1].
Это определение получило широкое признание среди медицинских работников и исследователей, занимающихся проблемой боли, и было принято Всемирной организацией здравоохранения. Данное определение также пережило различные критические замечания, высказанные экспертами по проблеме боли в середине—конце 1990-х годов.
Самой серьезной и обсуждаемой была критика определения боли, высказанная К. Анандом и К. Крейгом (K. Anand, K. Craig, 1996), которые поставили под сомнение вторую часть определения боли, связанную с необходимостью вербализации испытываемых человеком сенсорных и эмоциональных переживаний [2]. Они утверждали, что существующее определение боли неприменимо к людям, которые неспособны к самоотчету. В эту категорию вошли новорожденные, маленькие дети, умственно отсталые, пациенты с когнитивными нарушениями.
Критике также подвергалась и первая часть определения боли («неприятное сенсорное и эмоциональное переживание, связанное с повреждением тканей») как неспособная отразить все многообразие проявлений боли, особенно при повреждении периферических нервов. На эти трудности впервые обратил внимание Говард Филдс (Howard Fields, 1999): «Пациенты с повреждением нерва часто сообщают о незнакомых ощущениях и используют слова, которые не предполагают угрозы повреждения или самого повреждения» [3]. Известно, что некоторые формы невропатической боли могут иметь сенсорные и аффективные характеристики, которые не похожи на ноцицептивные боли, связанные с повреждением тканей.
В 2018 г. IASP сформировала многонациональную президентскую целевую группу из 14 экспертов, обладающих широким опытом в области клинических и фундаментальных исследований, связанных с проблемой боли, чтобы оценить определение боли, сформулированное в 1979 г., и дать рекомендации по сохранению или изменению этого определения. Через 2 года работы многопрофильной целевой группы IASP было предложено пересмотренное определение боли, которое опубликовано вместе с комментариями действующего президента IASP L. Arendt-Nielsen, а также экс-президента IASP J. Turner. В новом определении авторами были учтены многие нюансы и разнообразие болевых синдромов.
Ключевым изменением в новом определении боли по сравнению с версией 1979 г. является замена терминологии, которая основывалась на способности человека описать переживание таким образом, чтобы его можно было классифицировать как боль. Эксперты IASP подчеркивают, что боль не является простым сенсорным симптомом. Для оценки боли требуется комплексное обследование человека, учитывающее его когнитивные проблемы, психологические и социальные факторы, которые важны в лечении боли. Эксперты также отмечают, что в новом определении боли отражены знания о тех видах боли, которые не были описаны 40 лет назад. К таким видам болевых синдромов относится невропатическая и дисфункциональная боль.
Авторы нового определения боли считают, что изменения помогут врачам адекватно относиться к боли у детей, пожилых и старых людей со значительными когнитивными расстройствами, инвалидов, страдающих расстройством речи.
Рабочей группой IASP также были разработаны 6 пояснений к основному пересмотренному определению боли с целью повышения эффективности при оценке и лечении боли у пациентов:
— Боль — это всегда личное переживание, на которое в той или иной степени влияют биологические, психологические и социальные факторы.
— Боль и ноцицепция — разные явления. Боль не может быть следствием только активности сенсорных нейронов.
— Люди познают боль через свой жизненный опыт.
— Если человек сообщает, что ощущает боль, к этому нужно относиться с уважением.
— Хотя боль обычно играет адаптивную роль, она может оказывать неблагоприятное влияние не только на функции организма, но и на социальное и психологическое благополучие.
— Вербальное описание — это только один из нескольких способов выражения боли; неспособность общаться не отрицает возможности того, что человек или животное испытывает боль.
Пересмотренное определение и примечания были единогласно приняты Советом IASP в начале 2020 г. и опубликованы в журнале Pain [4].
В англоязычной версии новое определение боли выглядит следующим образом: «Pain is an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage».
Комитетом по терминологии Российского общества по изучению боли (РОИБ) были предложены для обсуждения экспертами следующие варианты перевода:
1. «Боль — неприятное сенсорное и эмоциональное переживание, связанное или схожее с тем, что связано с действительным или возможным повреждением тканей».
2. «Боль — неприятное сенсорное и эмоциональное переживание, связанное с действительным или возможным повреждением тканей или схожее с таковым переживанием».
3. «Боль — неприятное сенсорное и эмоциональное переживание, связанное с действительным или возможным повреждением тканей или напоминающее таковое переживание».
4. «Боль — неприятное сенсорное и эмоциональное переживание, связанное с имеющимся или перенесенным ранее действительным или предполагаемым повреждением тканей».
Первый вариант перевода сделан с учетом сохранения структуры оригинального предложения на английском языке: «…associated with, or resembling that associated with…» В переводе на русский язык такая конструкция предложения представляется не совсем правильной и может вызывать непонимание у читателей.
Четвертый вариант перевода логичен, однако имеет структуру, далекую от оригинала, и не может считаться определением, предложенным экспертами IASP.
В связи с этим руководителям комитетов РОИБ было предложено выбрать для утверждения русскоязычной версии перевода определения боли два варианта — 2-й и 3-й.
Большинство экспертов выбрали следующий вариант перевода определения боли: «Боль — неприятное сенсорное и эмоциональное переживание, связанное с действительным или возможным повреждением тканей или схожее с таковым переживанием».
Авторы заявляют об отсутствии конфликта интересов.